Projects | In Progress
Benefits of ICU Admission for Patients with Acute Respiratory Failure or Sepsis: A Mixed-Methods Study Across 26 Hospitals (ICU Net Benefit)
Research Areas
PAIR Center Research Team




Topics
Overview
Hospitalizations for patients with acute respiratory failure (ARF) and sepsis are common and costly. Special hospital floors called intensive care units (ICUs) were designed to care for patients who require life support, but they have since expanded to care for patients who do not require these therapies. It is unknown, among patients with sepsis and ARF who do not require life support, who receives a true benefit from receiving care in an ICU. Learning to care for these groups of patients on non-specialized hospital floors (such as a ward) would create healthcare system-wide benefits including better patient outcomes, reduced costs, and enhanced access to scare ICU resources for patients who need them the most. We conducted a retrospective study of over 135,000 patients admitted to 27 U.S. hospitals between 2013 and 2018 with sepsis and/or ARF who did not require life support in the emergency department. We measured the net benefit of ICU admission on patient outcomes including hospital length-of-stay and mortality. We used mixed methods to identify hospital characteristics and care processes that may contribute to observed benefits of ICU- or ward-based care.
Results & Impact
Choices to admit patients with ARF and/or sepsis to the ICU versus ward are associated with substantial differences in outcomes. On average, analyzing data combined across 27 hospitals showed patients with sepsis who do not require life support may have better outcomes, specifically a shorter time in the hospital and lower risk of dying in the hospital, when admitted to a ward for care. On average, analyzing data combined across 27 hospitals showed patients with ARF who do not require life support may have better outcomes (same as above) when admitted to an ICU for care. The size and direction of the difference in these outcomes for ARF and sepsis patients vary among hospitals. Cultural and communication factors were cited as main contributors by clinicians and administrators at hospitals where the highest benefits of ICU admission were observed. More work is needed to explain the observed outcome differences and apply these insights to improve care for patients with ARF and sepsis regardless of where they are treated.
-
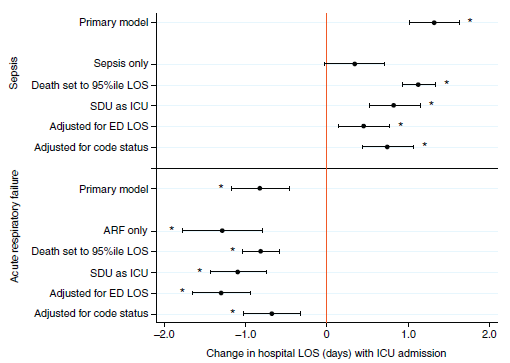
Association of ICU versus ward admission with hospital length of stay (LOS) among patients with sepsis and ARF. Among high-acuity patients with sepsis who did not require mechanical ventilation or vasopressors in the emergency department, admission to the ICU was associated with a 1.32-day longer hospital LOS. Among high-acuity patients with ARF who did not require mechanical ventilation or vasopressors in the emergency department, admission to the ICU was associated with a 0.82-day shorter hospital LOS. -
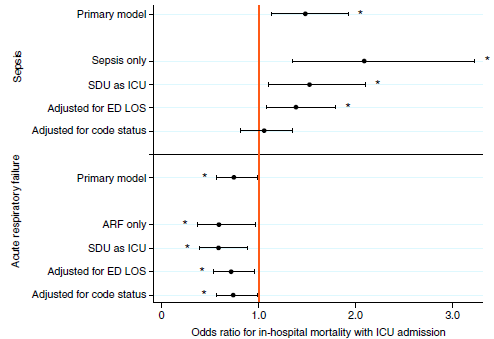
Association of ICU versus ward admission with in-hospital mortality among patients with sepsis and ARF. Among high-acuity patients with sepsis who did not require mechanical ventilation or vasopressors in the emergency department, admission to the ICU was associated with 48% increased odds of in-hospital mortality. Among high-acuity patients with ARF who did not require mechanical ventilation or vasopressors in the emergency department, admission to the ICU was associated with 25% decreased odds of in-hospital mortality.
Partnering Health Systems
Kaiser Permanente Northern California
Sponsors
National Heart, Lung, and Blood Institute